


Overview
Choosing between an Allied Health Assistant and a Support Worker can be confusing, especially when both roles may appear similar on the surface. While both provide valuable support under the NDIS, their responsibilities, qualifications, and impact on participant goals can be very different. In this guide, we'll break down the key differences, explain when each service may be appropriate, and help you understand how the right support can contribute to greater independence, mobility, and quality of life.
Table of contents
(28 sections)
Table of contents
(28 sections)Choosing between an Allied Health Assistant (AHA) and a Support Worker can be confusing especially if you're new to the NDIS. Although both roles provide valuable support, they serve very different purposes. Choosing the wrong one may affect your therapy outcomes, your NDIS funding, and even your long-term goals.
In this guide, we'll explain the differences in plain language so you can confidently choose the support that's right for you.
What Is an Allied Health Assistant?
If your physiotherapist has given you exercises to do at home but you struggle to stay consistent, an Allied Health Assistant can help you practise those exercises safely between appointments. The AHA does not assess, diagnose, or create treatment plans. Their defined function is to deliver clinically prescribed activities between a participant's appointments with their treating physiotherapist, occupational therapist, speech pathologist, or similar professional.
Qualifications and Training
AHAs complete a nationally recognised Certificate IV in Allied Health Assistance. This training prepares them to safely deliver therapy programs designed by physiotherapists, occupational therapists, and other allied health professionals.
Human anatomy and physiology as it applies to allied health contexts
Delivery of therapy programmes across physiotherapy, occupational therapy, and speech pathology
Safe manual handling, positioning, and use of assistive equipment for people with physical disability
Observation, measurement, and documentation of participant progress
Identification of deterioration and escalation protocols
Professional communication within multidisciplinary clinical teams
This is a structured clinical qualification. It cannot be substituted by general disability training or a Certificate III in Individual Support.
Clinical Supervision Requirements
Every AHA operating under the NDIS must work within a formal supervision arrangement with a registered allied health professional. This is not a matter of practice preference it is an NDIS requirement.
Under this structure, the supervising clinician:
Designs the therapy programme and specifies each component
Trains the AHA in programme delivery before sessions commence
Reviews session documentation submitted by the AHA
Adjusts the programme based on reported progress and clinical assessment
Retains professional and legal accountability for programme outcomes
Participants should always be able to identify the supervising clinician by name before AHA sessions begin. AHA support without an active supervision arrangement is not NDIS-compliant and carries clinical risk.
What Is a Support Worker?
A Support Worker assists NDIS participants with daily living tasks such as personal care, domestic assistance, community access, transport, meal preparation, and social participation. Their primary function is to support participants in maintaining their current routine, independence, and quality of life. Unlike an Allied Health Assistant, a Support Worker services focuses on helping you manage everyday life rather than delivering therapy.
Role and Responsibilities
Under the NDIS, Support Workers typically deliver:
Personal care: Showering, dressing, grooming, and hygiene support
Domestic assistance: Cleaning, laundry, and home safety maintenance
Meal preparation: Grocery shopping, cooking, and dietary support
Community access: Accompanying participants to appointments, activities, and events
Social participation: Supporting engagement with community programmes and social connections
Transport: Driving or accompanying participants to relevant destinations
Training and Scope of Work
Support Workers are not required to hold a formal clinical qualification under the NDIS. Many hold a Certificate III in Individual Support or Certificate IV in Disability, though neither is mandated. They do not operate within a clinical supervision structure, and they are not accountable to an overseeing allied health professional.
The scope distinction is important: a Support Worker assists a participant in completing daily tasks. An AHA trains, guides, and monitors a participant in working toward prescribed clinical goals. These are different functions, and they produce different outcomes.
AHA vs Support Worker: Core Differences
Allied Health Assistant | Support Worker | |
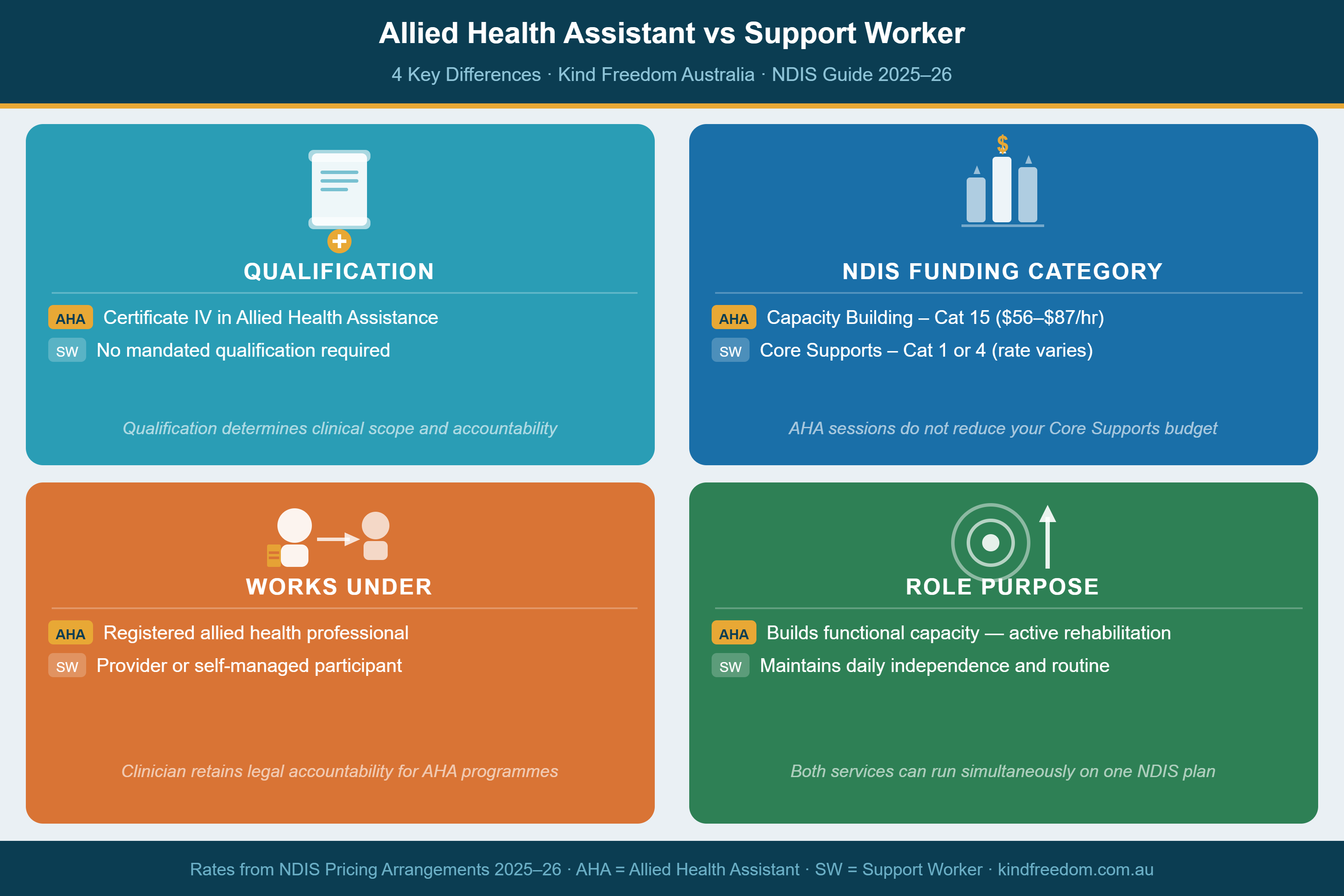
Qualification | Certificate IV in Allied Health Assistance | No formal requirement (varies by provider) |
Works under | Registered allied health professional | Provider organisation |
Deliver therapy programmes? | Yes, under clinical supervision | No |
Clinical accountability | Supervising allied health professional | Provider and NDIS Practice Standards |
Session documentation | Required, submitted to supervising clinician | Varies by provider |
NDIS funding category | Capacity Building, Improved Daily Living | Core Supports, Assistance with Daily Life |
Hourly rate (2025–26) | $56.16/hr | ~$35–$65/hr (time and complexity dependent) |
Best suited for | Rehabilitation, neurological conditions, post-acute recovery | Daily living, personal care, community access |
Can be NDIA-managed? | Registered providers only | Registered providers only |
How the NDIS Funds Each Role
One of the biggest differences between an Allied Health Assistant (AHA) and a Support Worker is how their services are funded under the NDIS.
Support Worker services are generally funded through Core Supports – Assistance with Daily Life, which covers everyday support such as personal care, household tasks, and community participation.
Allied Health Assistant (AHA) services are typically funded through Capacity Building – Improved Daily Living, as they focus on helping participants build skills and work towards therapy goals under the supervision of an allied health professional.
Because these are separate funding categories, using an AHA doesn't usually reduce the funding available for your regular Support Worker services.
If you're unsure which funding categories are included in your NDIS plan, speak with your plan manager, support coordinator, or service provider before starting supports. They can help you understand what funding is available and which services best match your goals.
When AHA Support Is Appropriate
AHA support is most clinically effective when a participant has active rehabilitation or therapy goals, a treating allied health professional overseeing a programme, and Capacity Building funding in their NDIS plan.
Neurological and Physical Disability Conditions
Multiple Sclerosis: People living with Multiple Sclerosis often benefit from regular therapy between physiotherapy appointments. An Allied Health Assistant helps participants safely practise their prescribed exercises at home while monitoring progress for the supervising physiotherapist.
Parkinson's Disease: Unlike an Allied Health Assistant, a Support Worker focuses on helping you manage everyday life rather than delivering therapy.
Acquired Brain Injury: Recovery following ABI is driven by neuroplasticity the brain's capacity to form new functional connections through structured repetition. An AHA delivers this repetition, aligned to OT and physiotherapy goals, in the environment where those functional gains must apply. The frequency and quality of practice between clinical sessions directly influences recovery outcomes.
Post-Stroke Recovery: After a stroke, practising exercises consistently is one of the biggest factors in recovery. An AHA helps participants continue those exercises correctly between therapy appointments, giving them more opportunities to regain movement and independence.
Spinal Cord Injury: Home exercise programmes for SCI require precise positioning, safe transfer techniques, and an understanding of the specific clinical risks that apply. An AHA trained in SCI support delivers these sessions safely and flags any changes in tone, sensation, or skin integrity to the clinical team without delay.
Cerebral Palsy: For adults with CP, AHA support provides structured maintenance of physiotherapy and OT gains, management of spasticity through prescribed programmes, and consistent work toward long-term independence goals. The frequency of AHA sessions sustains what clinical appointments alone cannot.
Post-Hospital Discharge and Recovery
The post-discharge period following a stroke, surgery, acquired injury, or acute illness represents one of the highest-risk and most clinically important windows for rehabilitation. Many participants leave hospital with a home programme but no structured support to deliver it between their first outpatient appointments.
An AHA can begin home programme delivery within the first week post-discharge, working directly from the inpatient rehabilitation team's prescription. This prevents the functional regression that commonly occurs when participants manage home programmes without clinical guidance.
Ongoing Support for Progressive Conditions
For participants with progressive neurological conditions, AHA support functions as a long-term clinical service rather than a short-term rehabilitation intervention. The AHA's ongoing session records provide the treating team with a longitudinal picture of functional change enabling timely programme adjustments and earlier escalation when deterioration is identified.
When a Support Worker Is the Right Choice
A Support Worker is the appropriate choice when a participant's primary need is consistent assistance with daily living rather than active therapy delivery.
This includes participants who:
Require personal care, domestic assistance, or meal support as part of their daily routine
Need support to access community activities, appointments, or social connections
Are in a stable phase where no active therapy programme is currently in place
Have therapy goals managed directly by their allied health team without a home programme component
Support Workers provide a consistent, person-centred daily presence that enables independent living for many people with disabilities. This is not a secondary or lesser service it is the correctly matched service for the support needed.
Participants recovering from an acute episode or entering a rehabilitation phase should discuss with their treating team whether AHA support should be added alongside their Support Worker arrangements.
Using Both Roles in One NDIS Plan
AHA and Support Worker services are not mutually exclusive and can be delivered simultaneously within the same NDIS plan, provided the plan includes both Core Supports and Capacity Building funding.
A typical combined arrangement:
Support Worker delivers personal care and community access four days per week (Core Supports — Category 1)
Allied Health Assistant delivers physiotherapy home programme twice per week (Capacity Building — Category 8)
Because these two roles draw from separate budget categories, they do not compete for the same funds. Participants who currently have Support Worker services only but are now pursuing active rehabilitation goals should raise the addition of Capacity Building funding at their next plan review. Documented evidence of therapy goals and an allied health professional's recommendation will support this request.
How an AHA Session Works
For participants new to AHA support, understanding the operational structure of sessions sets appropriate expectations.
Before sessions begin: The supervising allied health professional assesses the participant, establishes functional goals, and designs a home programme. They provide the AHA with a detailed programme handover covering the purpose of each activity, correct technique, safety considerations, and monitoring requirements.
Session commencement: The AHA confirms the participant's current state any changes in symptoms, pain levels, fatigue, or function since the previous visit. This check-in directly informs how the session proceeds.
Programme delivery: The AHA guides the participant through the prescribed programme, maintaining correct technique, monitoring response, and pacing the session appropriately. AHAs do not deviate from the prescribed programme without direction from the supervising clinician.
Post-session documentation: Session outcomes are recorded activities completed, participant performance, any observed changes. This documentation is submitted to the supervising clinician for review.
Programme review: The supervising clinician reviews progress at scheduled intervals, adjusting exercises, progressing goals, or modifying the programme based on AHA reports and their own clinical assessment.
This cycle prescribe, deliver, report, review is the clinical system that distinguishes AHA support from informal exercise assistance. Every component of the cycle must be functional for AHA support to produce the outcomes it is designed for.
Questions to Ask Before Committing
Before signing a service agreement with any AHA or Support Worker provider, obtain clear answers to the following.
For Allied Health Assistant providers:
Does the AHA hold a Certificate IV in Allied Health Assistance? Can you provide evidence?
Who is the supervising allied health professional for this participant's programme?
How frequently does the clinician review the programme and the AHA's session notes?
What is the exact support item number being claimed from the participant's plan?
How are session records documented and communicated to the treating team?
What is the process if the participant's condition changes between clinical appointments?
For Support Worker providers:
What training does this worker hold relevant to the participant's specific condition?
How does the provider ensure worker consistency for this participant?
What is the communication process if support needs change or the participant raises a concern?
Is a written service agreement provided before the first session?
How to Decide Which Support Is Right for You
The decision between AHA and Support Worker support comes down to two questions.
First: Is there an active therapy programme that requires delivery outside of clinical appointments?
If a physiotherapist, OT, or speech pathologist has prescribed a home programme and recommended a therapy assistant to implement it, the answer is AHA. If no active programme exists, the need is for daily living support and a Support Worker is the right fit.
Second: Does the current NDIS plan include Capacity Building Improved Daily Living funding?
AHA sessions must be billed from Category 8. If the plan does not include this budget, AHA sessions cannot be claimed in the current plan period. If the plan does not include it and an active therapy programme is in place, raising this at the next plan review with supporting documentation from the treating clinician is the appropriate next step.
If you are uncertain whether your current plan includes Capacity Building funding, your plan manager, support coordinator, or local area coordinator can confirm this from your plan document. The funding categories are listed clearly in all current NDIS plan documents.
Red Flags to Watch For
Not every provider offers the same level of quality or clinical oversight. Before choosing an Allied Health Assistant or Support Worker, watch for these common warning signs.
🚩 1. No Named Supervising Clinician (For AHA Services)
An Allied Health Assistant should always work under the supervision of a qualified allied health professional, such as a physiotherapist or occupational therapist.
If a provider cannot tell you who supervises the AHA or how that supervision works, it's a major red flag. Without proper clinical oversight, therapy programmes may not be delivered safely or in line with NDIS expectations.
🚩 2. Unclear Qualifications
Be cautious if a provider says things like "our staff are fully trained" without explaining what qualifications they actually hold.
For Allied Health Assistant services, ask whether the worker has completed a Certificate IV in Allied Health Assistance. A reputable provider should be happy to provide this information.
🚩 3. No Progress Notes or Session Documentation
AHA sessions should include clear documentation that is shared with the supervising clinician.
If the provider cannot explain how they record progress or communicate with the treating therapist, important changes in your condition could be missed.
🚩 4. Confusion About NDIS Funding
A trustworthy provider should clearly explain which NDIS budget their services will be claimed from.
If they're unsure whether AHA sessions come from Capacity Building – Improved Daily Living or suggest claiming them from Core Supports, ask for clarification before proceeding. Incorrect claims can create funding and compliance issues later.
🚩 5. No Written Service Agreement
Before services begin, you should receive a written service agreement outlining the support you'll receive, the costs, cancellation terms, and how services will be delivered.
If a provider wants to start services without any written agreement, consider it a warning sign and ask for the documentation first.
💡 Quick Tip: If a provider is transparent about their qualifications, supervision arrangements, documentation process, and NDIS funding, it's usually a good sign that they follow best practices. Don't be afraid to ask questions before signing a service agreement reputable providers will welcome them.
Common Mistakes People Make When Choosing Between an Allied Health Assistant and a Support Worker
Many participants accidentally choose the wrong type of support simply because the two roles sound similar. Here are some of the most common mistakes to avoid:
❌ Assuming an Allied Health Assistant and a Support Worker do the same job.
❌ Asking a Support Worker to deliver physiotherapy or occupational therapy exercises.
❌ Claiming Allied Health Assistant sessions from the wrong NDIS budget.
❌ Not asking who supervises the Allied Health Assistant.
❌ Choosing a provider based only on the hourly rate instead of qualifications and experience.
Understanding these differences can help you avoid funding issues, receive the right level of support, and achieve better outcomes from your NDIS plan.
AHA Support in Melbourne's Western Suburbs
If you're located in Melbourne's western suburbs and you're looking for either Allied Health Assistant support or daily living assistance, Kind Freedom provides both services with a strong focus on person-centred care, clinical collaboration, and helping participants work towards greater independence.
Our founder holds a Certificate IV in Allied Health Assistance and delivers AHA sessions in direct collaboration with participants' treating physiotherapists, occupational therapists, and specialists. We work with adults living with physical and neurological disability, including multiple sclerosis, spinal cord injury, acquired brain injury, stroke, Parkinson's disease, and cerebral palsy.
Kind Freedom supports self-managed and plan-managed NDIS participants. As an unregistered provider, we are unable to support NDIA-managed participants.
To discuss whether AHA support or daily living assistance is appropriate for your plan and current goals, contact us directly. No referral or obligation required.
Need Help Choosing the Right Support?
Choosing between an Allied Health Assistant and a Support Worker doesn't have to be confusing. If you're unsure which service best suits your NDIS goals, the team at Kind Freedom is here to help. We'll take the time to understand your needs, explain your options, and recommend the support that's right for you.
Contact us today hello@kindfreedom.com.au , 0405 458 852 to learn how our Allied Health Assistant and Support Worker services can help you achieve greater independence and reach your goals.
Written by
Edson Rushenya
Kind Freedom Australia blogger.
